The problem
Sponsors don't lack drugs. They lack a number at day one.
Oncology teams know intratumour heterogeneity matters — but ITH on a sequencing report rarely becomes a trial-actionable capacity score before first-line therapy starts.
Today that question is answered reactively: wait for progression, sequence the relapse, switch therapy, repeat. The Resistance Capacity Report answers it proactively from outputs already in the genomic report.
The deliverable
Two sequencing inputs. One plain-language report.
No new assay. No proprietary mutation panel. No trial-specific infrastructure.
ITH index
Fraction of somatic mutations that are subclonal — already reported by your sequencing vendor. Captures how much evolvable signal is present.
CCF variance
Variance in cancer cell fraction across subclonal clusters — from standard clonal architecture analysis. Captures evolutionary learning capacity.
Each patient receives a capacity tier with protocol implications:
How it works
Simple for your team. Rigorous under the hood.
-
1
Send a de-identified export Patient ID, ITH fraction, and CCF variance per assessment — a simple spreadsheet from your CRO or sequencing vendor.
-
2
We score and benchmark Each patient is assigned a capacity tier and compared against published NSCLC and cross-cancer reference profiles.
-
3
You receive a report Cohort summary, per-patient capacity tiers, plain-language interpretations, and recommended next steps for trial planning.
Public validation
Built on data sponsors already trust.
Fully anonymized case study using published aggregates and public cohorts — no client data required to evaluate the method.
TRACERx 421 NSCLC
r = 0.96
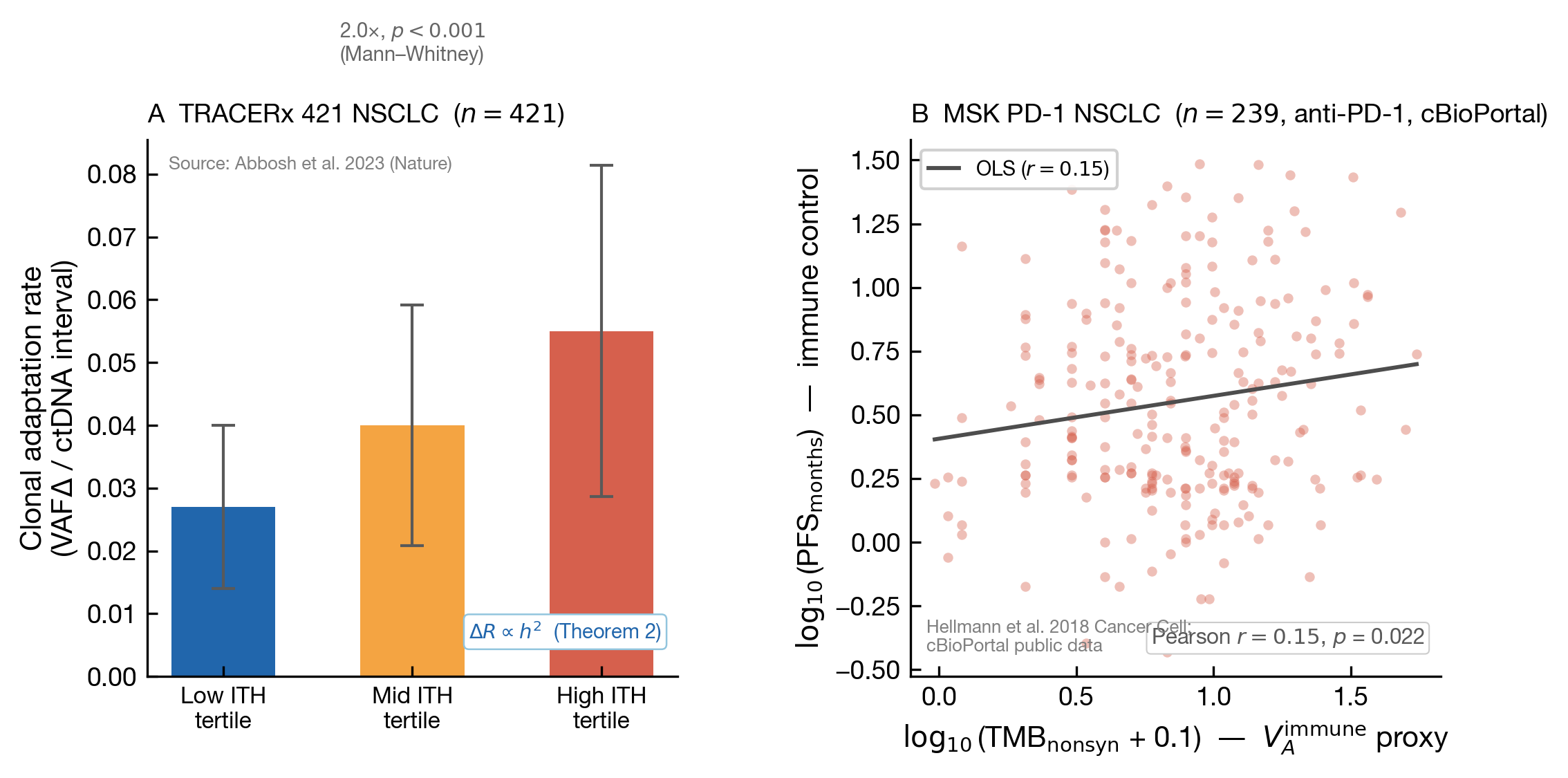
Validation from public data: TRACERx 421 clonal adaptation by ITH tertile (Abbosh et al. 2023) and MSK PD-1 NSCLC TMB–PFS association (Hellmann et al. 2018; cBioPortal).
Get started
Pilot programme
Fixed-fee engagement. De-identified intake. Report within five business days.